Abana dosages: 60 pills
Abana packs: 1 bottle, 2 bottle, 3 bottle, 4 bottle, 5 bottle, 6 bottle, 7 bottle, 8 bottle, 9 bottle, 10 bottle
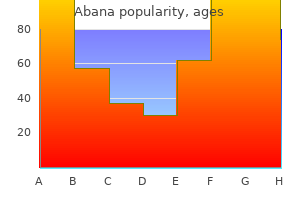
Generic abana 60pills otcThis randomized controlled trial confirms that the 2 cyclophosphamide regimens are associated with related remission induction rates and time to remission induction cholesterol in eggs white buy abana 60pills on line, with the heartbeat cyclophosphamide regimen leading to about one half the cumulative medicine dose of the oral routine and a considerably decrease fee of leukopenia cholesterol hdl ratio low generic 60pills abana visa. The long-term results would suggest that the every day oral cyclophosphamide regimen portends less relapse danger cholesterol foods pdf cheap abana online master card, and there was a trend towards this in the unique examine cholesterol medication that increases triglycerides abana 60 pills low price. At this point, clinicians must weigh the risks and benefits of both routine to determine which is most acceptable, and this decision could probably be based more heavily now on degree of affected person compliance. The length of cyclophosphamide remedy has modified significantly, largely based on the results of a big controlled trial by which patients who attained a whole remission with cyclophosphamide after 3 months of therapy had been randomly assigned to switch to azathioprine or to proceed taking cyclophosphamide for a total of 12 months. After 12 months, each teams acquired azathioprine upkeep remedy for a further 12 months. However, the use of plasmapheresis along with immunosuppressive remedy seems to be helpful within the subset of patients who require dialysis on the time of presentation. Patients who eventually are able to discontinue dialysis normally achieve this within three or 4 months of initiation of therapy. Methotrexate was additionally related to a significantly larger fee of relapse than was cyclophosphamide (69. The dose of methotrexate should be lowered in patients whose creatinine clearance is less than eighty mL/min, and its use is contraindicated when creatinine clearances is lower than 10 mL/min. Methotrexate is therefore unlikely to have any function in the remedy of pauci-immune crescentic glomerulonephritis alone. Whether using cyclophosphamide can be reduced or averted fully by method of rituximab has been the topic of two randomized controlled trials. The fee of sustained remission was similar in the two therapy groups (76% within the rituximab group vs. Severe adverse events had been widespread in each groups, affecting 45% of patients in the rituximab group and 36% in the cyclophosphamide group (P = 0. In a big managed trial designed to assess the noninferiority of rituximab in comparison with cyclophosphamide, 197 patients have been randomly assigned to treatment with either rituximab (375 mg/m2 infusions as soon as weekly � 4) or cyclophosphamide (2 mg/kg/day orally) for months 1 to three followed by azathioprine (2 mg/kg/day orally) for months four to 6. All patients obtained methylprednisolone (1 g/day intravenously for as a lot as 3 days) adopted by prednisone (1 mg/kg/day, tapered off fully by 6 months). The induction section of this trial revealed similar rates between the 2 remedy groups in complete remission at 6 months (64% within the rituximab group vs. Strategies for reducing therapy toxicity are being studied and are thought-about in higher element in Chapter 34. Ruggenenti P, Ruggiero B, Cravedi P, et al: Rituximab in steroiddependent or incessantly relapsing idiopathic nephrotic syndrome. Suzuki H, Fan R, Zhang Z, et al: Aberrantly glycosylated IgA1 in IgA nephropathy patients is acknowledged by IgG antibodies with restricted heterogeneity. Xiao H, Heeringa P, Hu P, et al: Antineutrophil cytoplasmic autoantibodies particular for myeloperoxidase trigger glomerulonephritis and vasculitis in mice. Levidiotis V, Freeman C, Tikellis C, et al: Heparanase is involved in the pathogenesis of proteinuria as a end result of glomerulonephritis. Jeansson M, Haraldsson B: Glomerular dimension and charge selectivity within the mouse after exposure to glucosaminoglycan-degrading enzymes. Garg P, Rabelink T: Glomerular proteinuria: a fancy interplay between distinctive gamers. Devarajan P: Mechanisms of orthostatic proteinuria: lessons from a transplant donor. Murakami S, Igarashi T, Hara S, et al: Strategies for asymptomatic microscopic hematuria: a potential research of 1,034 sufferers. Shen P, He L, Jiang Y, et al: Useful indicators for performing renal biopsy in adult patients with isolated microscopic haematuria. Pardo V, Riesgo I, Zilleruelo G, et al: the scientific significance of mesangial IgM deposits and mesangial hypercellularity in minimal change nephrotic syndrome. Fujimoto S, Yamamoto Y, Hisanaga S, et al: Minimal change nephrotic syndrome in adults: response to corticosteroid remedy and frequency of relapse. Koyama A, Fujisaki M, Kobayashi M, et al: A glomerular permeability issue produced by human T cell hybridomas. Kobayashi K, Yoshikawa N, Nakamura H: T-cell subpopulations in childhood nephrotic syndrome. Sasdelli M, Rovinetti C, Cagnoli L, et al: Lymphocyte subpopulations in minimal-change nephropathy. Sekhon I, Munjal S, Croker B, et al: Glomerular tip lesion associated with nonsteroidal anti-inflammatory drug-induced nephrotic syndrome. Horino T, Takao T, Morita T, et al: Minimal change nephrotic syndrome associated with systemic lupus erythematosus. Laurent J, Rostoker G, Robeva R, et al: Is adult idiopathic nephrotic syndrome meals allergy Kano K, Nishikura K, Yamada Y, et al: No impact of fluvastatin on the bone mineral density of children with minimal change glomerulonephritis and a few focal mesangial cell proliferation, aside from an ameliorating effect on their proteinuria. Ueda N: Effect of corticosteroids on some hemostatic parameters in kids with minimal change nephrotic syndrome. Groshong T, Mendelson L, Mendoza S, et al: Serum IgE in patients with minimal-change nephrotic syndrome. Lagrue G, Branellec A, Blanc C, et al: A vascular permeability consider lymphocyte tradition supernants from patients with nephrotic syndrome. Boulton J, Tulloch I, Dore B, et al: Changes within the glomerular capillary wall induced by lymphocyte products and serum of nephrotic patients. Maruyama K, Tomizawa S, Seki Y, et al: Inhibition of vascular permeability factor manufacturing by ciclosporin in minimal change nephrotic syndrome. Tomizawa S, Maruyama K, Nagasawa N, et al: Studies of vascular permeability issue derived from T lymphocytes and inhibitory impact of plasma on its production in minimal change nephrotic syndrome. Lagrue G, Xheneumont S, Branellec A, et al: A vascular permeability factor elaborated from lymphocytes. Toyabe S, Kaneko U, Hara M, et al: Expression of immunoglobulin E-dependent histamine-releasing consider idiopathic nephrotic syndrome of childhood. Kitano Y, Yoshikawa N, Nakamura H: Glomerular anionic sites in minimal change nephrotic syndrome and focal segmental glomerulosclerosis. Acharya B, Shirakawa T, Pungky A, et al: Polymorphism of the interleukin-4, interleukin-13, and sign transducer and activator of transcription 6 genes in Indonesian youngsters with minimal change nephrotic syndrome. Berdeli A, Mir S, Ozkayin N, et al: Association of macrophage migration inhibitory factor -173C allele polymorphism with steroid resistance in children with nephrotic syndrome. Ponticelli C, Passerini P: Treatment of the nephrotic syndrome associated with main glomerulonephritis. Nephrotic syndrome in children: a randomized trial evaluating two prednisone regimens in steroid-responsive sufferers who relapse early. Alternate-day versus intermittent prednisone in regularly relapsing nephrotic syndrome. Leisti S, Hallman N, Koskimies O, et al: Association of postmedication hypocortisolism with early first relapse of idiopathic nephrotic syndrome. Leisti S, Koskimies O, Perheentupa J, et al: Idiopathic nephrotic syndrome: prevention of early relapse. Leisti S, Koskimies O: Risk of relapse in steroid-sensitive nephrotic syndrome: effect of stage of post-prednisone adrenocortical suppression. Short versus normal prednisone remedy for preliminary therapy of idiopathic nephrotic syndrome in youngsters. Cyclophosphamide remedy of steroid dependent nephrotic syndrome: comparison of eight week with 12 week course. Effect of cytotoxic drugs in incessantly relapsing nephrotic syndrome with and without steroid dependence. Ueda N, Kuno K, Ito S: Eight and 12 week courses of cyclophosphamide in nephrotic syndrome. El-Husseini A, El-Basuony F, Mahmoud I, et al: Long-term results of cyclosporine in youngsters with idiopathic nephrotic syndrome: a single-centre expertise. Iyengar A, Karthik S, Kumar A, et al: Cyclosporine in steroid dependent and resistant childhood nephrotic syndrome. Nakahata T, Tanaka H, Tsugawa K, et al: C1-C2 point monitoring of low-dose cyclosporin A given as a single daily dose in children with steroid-dependent relapsing nephrotic syndrome. Rinaldi S, Sesto A, Barsotti P, et al: Cyclosporine remedy monitored with abbreviated area beneath curve in nephrotic syndrome. Primary nephrotic syndrome in kids: medical significance of histopathologic variants of minimal change and of diffuse mesangial hypercellularity.
Diseases - Congenital adrenal hyperplasia due to 21-hydroxylase deficiency
- Acute myeloblastic leukemia type 3
- Beta ketothiolase deficiency
- Blepharophimosis syndrome Ohdo type
- Myelodysplastic syndromes
- Germinal cell aplasia
- Xerostomia
- Kuster syndrome
- Lower mesodermal defects
- Acyl-CoA dehydrogenase, medium chain, deficiency of
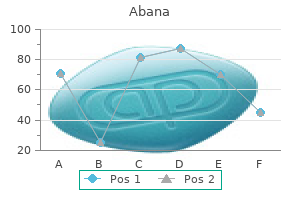
Generic 60 pills abana free shippingThe mechanism that predominates is probably related to the specific renal lesion causing the nephrotic syndrome cholesterol levels in child order 60pills abana with amex. Regardless of which mechanism happens initially good cholesterol definition buy abana 60 pills with visa, both will likely progress to a steady-state situation during which the effective arterial volume standing that initiated the disorder is troublesome or impossible to discern mg of cholesterol in shrimp order genuine abana line. Whether the initiating occasion is underfill of the effective arterial house cholesterol levels over 300 buy generic abana 60 pills line, resulting in renal salt and water retention, or overfill of this compartment, inflicting excess salt and water to enter the interstitial spaces, the development of clinically obvious edema in an adult requires the net retention of about 4 to 5 kg of fluid, which is equal to 4 to 5 L of normal saline. When the thumb is pushed towards a bony construction such as the tibia or sacrum, the ensuing pit stays seen for a brief time frame. Pitting edema is graded on a scale of 1 to four (from very slight to extra obvious to deep pitting that persists for >2 minutes). The interstitial strain in numerous areas has a significant influence on edema formation. Thus, the low ambient interstitial strain often results in outstanding periorbital edema. Gravitational forces additionally trigger nephrotic edema to accumulate in dependent body parts. Edema is usually worse within the lower legs and feet on the finish of the day and turns into extra prominent in the face after nocturnal recumbency. The diurnal variation of edema formation turns into much less outstanding when the degree of edema worsens. Nephrotic edema is often symmetric (after adjustment for gravitational dependency), and unilateral edema should increase the potential for native anatomic abnormalities, such as venous thromboses, varicosities, or lymphatic obstruction. However, uneven nephrotic edema may result from an anatomic situation that generates greater local or uneven edema. Chronic (months to years) severe edema of any cause, together with nephrotic syndrome, can produce fibrosis of the pores and skin and subcutaneous tissues. Physical clues to other problems that produce generalized edema should be sought throughout physical examination. The neck veins must be carefully evaluated to decide whether right-sided cardiac pressures are increased because of cardiac, pulmonary, or pericardial abnormalities. Although prominent ascites usually signifies liver illness, and pulmonary congestion and pleural effusions recommend cardiac or pulmonary pathology, fluid might accumulate in every of these places in sufferers with severe nephrotic syndrome in the absence of cardiac or hepatic abnormalities. Xanthelasma palpebrarum (periorbital-eyelid xanthomas) is commonly associated with hypercholesterolemia and should become very outstanding in nephrotic patients. Much rarer are eruptive xanthomas, usually associated with excessive hypertriglyceridemia, which may additionally occur with nephrotic syndrome. A number of relatively particular skin, nail, and scalp abnormalities are associated with numerous rheumatologic conditions that may cause the nephrotic syndrome. These include a malar facial rash, scarring alopecia, mat telangiectasia, nail mattress telangiectasia and nail fold capillary loops and vascular infarcts, and erythema nodosum. Sarcoidosis, which sometimes causes nephrotic syndrome, is related to erythema nodosum and skin papules. Jaundice, angiomata, telangiectasia, and palmar erythema raise the likelihood of hepatic problems. The vasculitides produce a variety of skin manifestations, including leukocytoclastic rashes and pores and skin infarctions. Nail-patella syndrome-characterized by dystrophic nails, hypoplastic patellae, and iliac horns-may present with nephrotic syndrome. The eyes, along with being swollen, may be inflamed or present evidence of scleritis with systemic vasculitic disease. The extremities should be fastidiously evaluated for proof of arthritis and for deep vein thrombi, which happen with elevated frequency in these patients. The protein-detecting pad is impregnated with a protein-sensitive pH indicator dye and a powerful pH buffer, which retains the pH of the wetted pad fixed and impartial of the urine pH. These pH indicators change shade when moistened with urine containing dissolved proteins, a phenomenon known as the protein error of pH indicators. Dipstick protein tests are most sensitive to albumin and react much less with urine globulins and immunoglobulin mild chains (Bence Jones protein). Dipstick outcomes have the following approximate correlations with protein concentration: � Negative: <15 mg/dL � Trace: 15-30 mg/dL Extremely alkaline urine. More lately, albumin-specific urine dipstick checks have been marketed specifically to detect low-grade albuminuria. Some additionally simultaneously measure creatinine concentrations (semiquantitatively) so that the urine albumin/creatinine ratio may be estimated. Albumin-specific dipstick tests are typically not used to diagnose or follow sufferers with overt albuminuria (macroalbuminuria) or nephrotic syndrome. Another methodology for urine protein determination is its response with sulfosalicylic acid, which precipitates most urine proteins. The sulfosalicylic acid turbidity check detects albumin, globulins, and Bence Jones proteins. If a high urine protein focus is documented, a quantitative measurement of protein excretion will be required. Alternatively, the protein/creatinine concentration ratio (protein/creatinine) in a morning specimen may be used. A timed quantitative urine collection has the benefit of permitting a simultaneous measurement of creatinine clearance. Urine dipstick protein checks, sulfosalicylic acid turbidity, 24-hour protein excretion, and protein/creatinine ratio are all measures of protein concentration or excretion. None of those exams will characterize the precise urine proteins (except that the urine dipstick checks are extra sensitive to albumin, and the albumin dipsticks are specific to that protein). Agarose gel protein electrophoresis of the urine separates the urine protein lessons (albumin, 1-globulin, 2-globulin, -globulin, -globulin), and permits identification of monoclonal immunoglobulins and light-weight chains. Electrophoresis results also allow stratification of nephrotic patients into these with selective proteinuria (mainly albumin) and people with nonselective proteinuria (highgrade albuminuria and globulinuria). Characterization of intact immunoglobulins, heavy chains, and lightweight chains is achieved with immunoelectrophoresis or immunofixation. Hyaline casts are common in patients with nephrotic syndrome and are composed primarily of precipitated TammHorsfall protein, with a small fraction of some abnormally filtered and excreted serum proteins. When medical and historical options are suggestive, cryoglobulin and antistreptolysin O titers must be obtained. A renal sonogram with Doppler study is required to determine the renal anatomy and standing of the collection system and renal vasculature. The finding of a single kidney, asymmetric kidney size, or bilaterally small kidneys will direct the following analysis. Patients ought to have routine age-indicated screening studies for malignancy, similar to mammography and colonoscopy. Visible lipids within the urine sediment could be seen in excreted tubule cells (oval fats bodies), inside fatty casts, and/or as free-floating lipid globules. Some of the urine fat originates from filtered high-density lipoprotein, which is small enough to be filtered by leaky glomeruli and is then partially reabsorbed by renal tubule epithelial cells. The sodium concentration may be artifactually decreased (pseudohyponatremia) on account of a displacement error caused by hyperlipidemia. This error happens when the sodium focus is measured by flame photometry or oblique potentiometry but not by analyzers using direct potentiometry. The calcium focus have to be corrected for the low albumin concentration, and direct measurement of the ionized calcium focus may be useful. If the trigger seems obvious from the historical past and laboratory studies, treatment can be initiated with out histologic confirmation. In younger children with a traditional medical and biochemical presentation, the prognosis of minimal change disease can usually be assumed and remedy initiated with out histologic affirmation. This explicit analysis is far less frequent in adults, so empirical therapy is much less generally initiated in these sufferers. In most adults with nephrotic syndrome, however, a biopsy is indicated to define the illness, improve prognostication, and direct therapeutic intervention. Prostatic enlargement and different prostate pathology, corresponding to malignancy or infection, may be detected via rectal examination. In an older woman, a cautious pelvic examination must be carried out to establish severe uterine prolapse, which has been reported to cause extreme hydroureteronephrosis.
Order discount abana onlineIn addition cholesterol flow chart buy abana 60 pills on line, it have to be borne in thoughts that low start weight and prematurity additionally predict later-life diabetes test cholesterol jean coutu order abana now, cardiovascular disease cholesterol on blood test results abana 60pills on line, and metabolic syndrome boost good cholesterol foods cheap 60 pills abana with mastercard, so renal function could also be additionally impacted via developmental programming of these organ techniques and, in turn, have an effect on outcomes of those diseases, the discussion of which is beyond the scope of the current chapter. Ongoing work is required to develop extra delicate measures of developmental stress. Globally, the respective incidences of low birth weight and prematurity are round 15% and 9. The relationship between renal sodium dealing with, intravascular quantity homeostasis, and hypertension is well accepted. This speculation was attractive in that an affiliation between a decreased nephron quantity and low birth weight, for example, may clarify differences in hypertension and renal illness prevalence noticed in populations of different ethnicity, amongst whom those who are inclined to have decrease delivery weights usually have a greater prevalence of hypertension and renal disease. In common, numbers of viable glomeruli are reduced in kidneys from older topics, owing to age-related glomerulosclerosis and obsolescence. Consistent with this notion, kidneys from rats that underwent unilateral nephrectomy at 3 days of age confirmed an identical complete glomerular number but a considerably smaller number of mature glomeruli in the remaining kidney than kidneys from people who underwent nephrectomy at one hundred twenty days of age. Numerous animal models have demonstrated the association of low birth weight (induced by gestational publicity to low-protein or low-calorie diets, uterine ischemia, dexamethasone, or vitamin A deprivation) with subsequent hypertension. As proven, the association between birth weight, nephron numbers, and blood pressures varies among models, underscoring the complexity of developmental programming and the necessity for better markers than birth weight. Vehaskari and colleagues demonstrated an nearly 30% discount in glomerular quantity in offspring of pregnant rats fed a low-protein diet in comparison with those fed a normal-protein food plan throughout being pregnant. Caucasian Australians50 Senegalese Africans372,388 Maternal vitamin A deficiency389 Indian vs. Not surprisingly, in animal research, timing of the gestational insult has been found to be crucial in renal programming, with the best influence on nephron quantity occurring during periods of most lively nephrogenesis. A kidney beginning with a lower nephron number, due to this fact, would conceivably attain a crucial discount of nephron mass, either with age or in response to a renal insult, sooner than a kidney with a greater nephron complement, predisposing to hypertension and/or renal dysfunction. Nephrogenesis in humans begins in the course of the ninth week of gestation and continues until the thirty fourth to thirty sixth week. It is mostly believed that no new nephrons are formed in people after time period start. To investigate whether or not glomerulogenesis does proceed postnatally in untimely infants, Rodriguez and colleagues studied kidneys at post-mortem from fifty six extremely untimely infants and compared them with kidneys of 10 full-term infants as controls. Furthermore, proof of energetic glomerulogenesis, indicated by the presence of S-shaped our bodies immediately under the renal capsule, was seen in premature infants who died before 40 days however was absent in those who died after 40 days of life, suggesting that nephrogenesis might continue for up to 40 days after untimely delivery. These investigators also stratified their instances by presence or absence of renal failure. This cross-sectional observation may counsel that renal failure inhibited glomerulogenesis or, conversely, that the presence of fewer glomeruli lowered the brink for development of renal failure in these infants. Those premature infants surviving longer than 40 days without renal failure exhibited glomerulomegaly, which may reflect, a minimum of in the brief time period, a compensatory renoprotective response. Faa and colleagues additionally reported evidence of lively glomerulogenesis in kidneys of untimely infants and two term infants who died at delivery, but not in a baby who died at age three months, suggesting that glomerular maturation may continue for a brief period even after time period delivery. These studies all help the hypothesis that an antagonistic intrauterine environment, which can manifest as low delivery weight or prematurity, is related to a congenital discount in nephron endowment and an early, compensatory increase in glomerular quantity. In a population of a hundred and forty adults aged 18 to sixty five years who died of various causes, a major correlation was additionally observed between delivery weight and glomerular number. Significantly, nevertheless, not one of the subjects in this research had been of low birth weight; subsequently, no conclusion may be drawn as to whether or not an affiliation between low birth weight and nephron number existed in either population group. B, Birth weight (top) and glomerular quantity (bottom) plotted towards glomerular quantity in neonates. Br J Obstet Gynaecol 99:296-301, 1992; B from Manalich R, Reyes L, Herrera M, et al: Relationship between weight at delivery and the number and dimension of renal glomeruli in people: a histomorphometric examine. Among term neonates, renal parenchymal thickness, proposed as a more accurate screening software than renal volume estimation, was significantly reduced in these with low compared to regular start weights. In one examine, supplementation of a low-protein food plan throughout gestation with glycine, urea, or alanine resulted in a normalization of nephron number in rat offspring, however blood strain normalized solely in those supplemented with glycine. Later evidence has proven alterations in renal tubular sodium dealing with and vascular perform in developmentally programmed kidneys that likely additionally contribute to later-life blood stress and renal perform changes as listed in Table 23. A reduction in filtration surface area associated with a reduction in nephron quantity is one believable speculation to explain the related greater blood pressures. Consistent with this association, salt sensitivity has been reported in a number of animal fashions to be related to low start weight and reduced nephron number. Expression and activity of renal tubule sodium transporters has due to this fact been investigated. J Am Soc Nephrol 16:2545-2556, 2005; B from Dagan A, Habib S, Gattineni J, et al: Prenatal programming of rat thick ascending limb chloride transport by low-protein food regimen and dexamethasone. Importantly, nonetheless, in some animal fashions, low nephron numbers have been observed also within the setting of normal start weight (see Table 23. In assist of the function of altered podocyte physiology in renal disease progression, related findings were observed within the Munich Wistar Fr�mter rat, a strain that has congenitally lowered nephron numbers and demonstrates spontaneous renal illness. The role of podocyte depletion, either absolute (loss of podocytes) or relative (podocyte density), in illness development deserves extra research focus, and currently nothing is thought about the possible results of developmental programming on podocyte endowment. Control teams (triangles); diabetes groups (circles); diabetes+insulin group (squares). The definitive pathophysiologic impact of a reduction in nephron quantity on the development of renal dysfunction is tough to elucidate from the present literature, which contains research using very varied experimental situations. A systematic review of 10 research evaluating premature subjects with these born at time period discovered that in untimely topics, having a imply gestational age of 30. Given that impact estimates for danger of upper blood pressures were related in the meta-analyses and systematic evaluations cited previously, nevertheless, at present each conditions should be deemed essential danger elements for subsequent high blood pressure. New subgroup 2500g Events Total 2500g Events Total upward crossing of weight percentiles), highlighting the significance of early postnatal diet in developmental programming. Another potential risk issue for greater offspring blood stress is maternal gestational hypertension or preeclampsia. The pooled odds ratios are proven as diamonds; 95% confidence intervals are in rackets. Top, Studies that adjusted for attained measurement; middle, Studies of solely very preterm or very low-birth-weight topics; bottom, higher-quality research. Similarly, among a subset of 63 topics in whom mean arterial pressures and birth weights have been out there, Hughson and coworkers reported a significant correlation between start weight and glomerular number, mean arterial pressure and glomerular quantity as well as mean arterial stress and delivery weight among the white but not African American topics. Glomerular volumes have been found to be greater among the hypertensive African American subjects than in the hypertensive whites. Among 1512 topics aged 62 years, investigators found an inverse association between birth weight and blood strain among those with birth weights less than 3050 g, with a progressive 2. With time or exposure to further insults, nevertheless, these changes may manifest as kidney illness. Reduced renal practical reserve was also observed amongst young adults with kind 1 diabetic moms, who had been uncovered to diabetes during gestation, however not those with diabetic fathers, once more suggesting a programming quite than genetic effect. The relative contributions of genetics and the fetal surroundings on programming of renal operate had been investigated in 653 twins. Consistent with this speculation, in Aboriginal Australians who had low delivery weights, the odds ratio for macroalbuminuria was 2. Among kids aged four years who had been premature, albuminuria was greater in each boys and girls who had reached regular height (presumably caught up in growth), and among 19-year-olds who had been very preterm, albuminuria was larger among those that had been growth restricted, once more showing the interplay between prematurity, development restriction, and catch-up growth and later threat of disease. This observation emphasizes the need for surrogate markers in addition to birth weight, so as to establish individuals at risk for renal programming. A U-shaped association between birth weight and proteinuria was described among Pima Indians, exhibiting that the danger elevated for birth weights lower than 2. The statistical size of the examine was defined when it comes to the inverse of the variance of the regression coefficient, indicated by gray squares. Dashed vertical line, the inverse variance-weighted regression by way of the general point estimate. Exposure measured as �exposure to famine midgestation (versus not exposed) and ponderal index within the lower third percentile (versus highest 3rd). F, Ultrastructural examination of glomerular capillary demonstrating podocyte foot process effacement (electron micrograph). In many of the experimental fashions of programming, reduced nephron quantity has been proven to be related to low birth weight and subsequent hypertension and renal harm. Interestingly, in normal rat litters, those pups with naturally occurring low birth weight. Maternal factors that have an result on start weight and prematurity in humans might therefore also affect nephrogenesis.
Buy cheapest abanaThe most typical cause for postrenal azotemia is structural or functional obstruction of the bladder neck cholesterol levels over 600 generic abana 60 pills. The fee and magnitude of useful restoration relies on the extent and period of the obstruction cholesterol test kit walmart cheap 60pills abana free shipping. Clinically patients can present with pain and oliguria cholesterol levels range australia order 60pills abana with visa, though these are neither specific nor delicate cholesterol test new zealand buy discount abana on-line. Early analysis and prompt aid of obstruction stay key targets in stopping long-term parenchymal damage because the shorter the interval of obstruction, the better the probabilities for recovery and favorable long-term outcomes. The pathophysiology and therapy of obstructive uropathy are mentioned extensively in Chapter 38 (see Table 31. Limitations in most experimental fashions embrace the dearth of comorbid conditions. We will briefly describe the pros and cons of using presently characterised experimental models Table 31. The parenteral supply of prophylactic therapeutic agents is unimaginable in full occlusion fashions. Total blood flow cessation additionally prevents the degradative merchandise of the ischemic kidney from being washed out. In the isolated perfused kidney model, the kidney is perfused ex vivo using perfusates with and with out erythrocytes, and the model employs either ischemic (stopping perfusate) or hypoxic (reduced oxygen tension of erythrocytes) to induce functional impairment. The morphologic patterns are totally different in erythrocyte-free and erythrocyte-rich perfusates. Additionally, limitations include exclusion of varied inflammatory mediators, neuroendocrine hemodynamic regulation, and systemic cytokine and growth issue interactions recognized to be current and play a pathophysiologic position in animal models and certain in human ischemia. Recently Burne-Taney and colleagues described a whole-body ischemia-reperfusion damage model induced by 10 minutes of cardiac arrest, followed by cardiac compression resuscitation, air flow, epinephrine, and fluids that result in a significant rise in serum creatinine level and renal tubular injury at 24 hours. Toxic models of kidney failure employ numerous identified toxins, similar to radiocontrast media, gentamicin, cisplatin, glycerol, and pigments, together with myoglobin and hemoglobin. The endotoxin model, which is easy, cheap, and appropriate for finding out new pharmacologic agents, has sure drawbacks as properly. Most typically, the agent is administered late in the midst of the human disease; affected person heterogeneity and the difficulty in stratifying patients by severity of damage makes it even more troublesome to establish efficacy. Of the three segments (S1 to S3), the S3 phase of the proximal tubule in the outer stripe of the medulla is the cell most susceptible to ischemic damage for several reasons. The S1 and S2 segments are mostly involved in poisonous nephropathy due to their high rates of endocytosis, leading to elevated mobile uptake of the toxin. Morphologic Changes vesicle remnants, and mobile debris together with Tamm-Horsfall glycoprotein kind the classical "muddybrown granular" casts. Frank necrosis itself is inconspicuous and restricted to the highly vulnerable outer medullary areas. Alternatively, options of apoptosis are extra generally seen in each proximal and distal tubular cells. Microvilli disruption and detachment from the apical cell surface forming membrane-bound blebs happens early with release into the tubular lumen. Actin microfilaments are formed by self-assembly of globular or G-actin into filamentous F-actin. The main pathways of impairment of glomerular filtration rate in ischemic acute tubular necrosis as a result of vascular and tubular injury (see textual content for details). The biopsy specimen, obtained inside 24 hours from a patient with exercise-induced rhabdomyolysis, revealed vital proximal tubular cell injury with intraluminal accumulation of apical membrane fragments and indifferent cell (*), thinning of proximal tubular cells to maintain monolayer tubule integrity (arrowhead), and dividing cells and accumulation of white cells throughout the microvascular area in the peritubular area (arrow). The patient required renal alternative therapy but did regain complete renal operate finally. Concomitantly, the focus of F-actin in the cell increases with the formation of enormous cytosolic aggregates within the perinuclear region and near the junctional complexes of the basolateral membranes. Other proteins involved in the depolymerization course of are tropomyosin and ezrin. Specifically, it has been proven that during ischemia ezrin, an actin-binding phosphorylated protein, turns into dephosphorylated, and the attachment between the microvillar F-actin core and the plasma membrane is lost. These junctional complexes actively participate in quite a few features, including paracellular transport, cell polarity, and mobile form. In sublethal ischemia the pumps redistribute to the apical membrane of the proximal tubule. Early ischemic harm ends in "opening" of these tight junctions, resulting in increased paracellular permeability causing further backleak of the glomerular filtrate into the interstitium. Integrins are transmembrane proteins normally answerable for the anchoring of epithelial cells to the substrate matrix through the actin cytoskeleton. The exfoliated cells can then exhibit irregular adhesions inside the tubular lumen among themselves, forming mobile casts throughout the tubular lumen as mentioned earlier. Postulated mediated mechanisms embody hyperphosphorylation of the protein ankyrin, with consequent loss of the binding protein spectrin, and cleavage of spectrin by activation of proteases similar to calpain. Investigators directly studied these responses through the use of fluorescent cytopathologic E. Tissue concentrations of cytokines, elevated within the affected space in comparability with none within the injected areas, revealed marked increases. Increasing durations of ischemia lead to more severe cell damage and longer recovery periods. With progressive approaches the chance of extratubular stem or progenitor cell populations migrating into the tubule was minimized or eliminated utilizing chimera and genetic fate� tracing methods. These information provide additional evidence that terminally differentiated epithelia are able to proliferate, and there was no evidence for an intratubular stem cell population. Cells present process sublethal or less severe harm have the capability for functional and structural recovery if the insult is interrupted. Cells that suffer a extra extreme (or lethal) injury undergo apoptosis or necrosis, leading to cell demise. Apoptosis is an energydependent, "programmed" cell dying after damage that leads to condensation of nuclear and cytoplasmic material, forming apoptotic our bodies. These apoptotic our bodies, that are plasma-membrane certain, are quickly phagocytosed by macrophages and neighboring viable epithelial cells. The caspase family of proteases has now been identified to be an necessary initiator in addition to an effector of apoptosis. There additionally exists considerable crosstalk between the intrinsic and extrinsic pathways. The other group of caspases, three, 6, and seven, are effector caspases, that are more ample and catalytically robust, cleaving many cellular proteins, ensuing within the classical apoptotic phenotype. It has additionally been proven that the balance between cell survival and death depends on the relative concentrations of the proapoptotic (Bax, Bcl-2�associated demise promoter [Bad], and Bid) and antiapoptotic (Bcl-2 and Bcl-xL) members of the Bcl-2 household of proteins. Overexpression of proapoptotic or relative deficiency of antiapoptotic proteins could result in formation of mitochondrial pores. Conversely, the inhibition of such pore formation may happen with the other imbalance. Overall, these results point out miR-24 promotes renal ischemic injury by stimulating apoptosis in endothelial and tubular epithelial cells. Apoptosis-activating factor is activated by cytochrome c, which binds to and prompts procaspase-9. Caspase-3 is activated by activated caspase-9, which along with different downstream caspases induces proteolysis of various cytosolic and nuclear proteins. Active caspase-8 activates caspase-3 and cleaves proapoptotic protein Bid to its truncated form tBid, which acts through Bax to induce cytochrome c from the mitochondria. Hence the extrinsic pathway also amplifies the occasions induced by the intrinsic pathway. Increased cytosolic calcium causes additional mitochondrial damage and cytoskeletal alterations. Phospholipases similar to phospholipase A2 cause direct hydrolytic injury to membranes and in addition launch poisonous free fatty acids. They additionally trigger release of eicosanoids that have vasoactive and hemokinetic actions, leading to an intense surrounding inflammatory response. Calpain mediates plasma membrane permeability, in addition to hydrolysis of the cytoskeleton proteins.
Pimenta (Allspice). Abana. - Are there any interactions with medications?
- Dosing considerations for Allspice.
- Are there safety concerns?
- Intestinal gas, stomachache, vomiting, diarrhea, purging the bowels, fever, flu, colds, heavy menstrual bleeding, and other conditions.
- How does Allspice work?
- What is Allspice?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96125
Generic abana 60pills on-lineThe reabsorption of citrate predominantly happens from the proximal convoluted tubule and foods to lower cholesterol levels quickly discount abana 60pills without a prescription, to a lesser extent cholesterol test cape town buy cheap abana 60 pills line, the proximal straight tubule cholesterol lowering diet books order abana line. Oxalate is a dicarboxylic acid and cholesterol medication list generics discount abana american express, in mammals, is an finish product of hepatic metabolism. Oxalate balance consists of ingestion and endogenous manufacturing versus intestinalandurinaryexcretion. A variety of different metabolic precursors of oxalate metabolism, together with by-products of the breakdown of ascorbic acid, fructose, xylose, and hydroxyproline, potentially contribute to oxalate production. However, their contribution beneath regular physiologic circumstances has not yet been totally elucidated. There is a large variation in estimated intake of oxalate, ranging from 50 to 1000 mg/day. The relationship between oxalate absorption and dietary oxalate intake has been demonstrated to be nonlinear. It was proposed that the primary fraction of oxalate is absorbed within the small gut, since most oxalate is absorbed during the first four to eight hours after the consumption of oxalate-rich meals,358,366,379,380 and 5 hours of intestinal transit time is required for vitamins to transfer from the stomach to the colon. Nevertheless, it has additionally been suggested that the colon additionally participates, however to a lesser extent, in oxalate absorption. However, it has been proposed that at a low gastric pH, part of the dietary oxalate is converted into small hydrophobic molecules that would probably diffuse via the lipid bilayer,381-384 thereby rising urinary oxalate excretion. The anion change transporter Slc26a6 has been shown to be involved in intestinal oxalate transport. Furthermore, in vivo studies in Slc26a6 null mice on a controlled oxalate diet confirmed increased plasma oxalate focus, decreased fecal oxalate excretion concentration, and excessive urinary oxalate excretion. These results counsel that diminished internet oxalate secretion in the gut is responsible for web oxalate absorption; this results in a rise in plasma oxalate focus, elevated urinary oxalate excretion and bladder stones, and Yasue-positive crystals in the kidney. However, the influence of this putative anion change transporter on intestinal oxalate absorption- particularly, its role in kidney stone formation in humans- has not but been demonstrated. Studies with exogenous radiolabelled oxalate in regular people have proven that renal excretion accounts for many of the disposal of oxalate. With impaired kidney perform, plasma oxalate focus steadily will increase, exceeds its saturation within the blood, and therefore enhances the chance of systemic tissue oxalate deposition, including kidney damage. Radiolabeled oxalate studies398,399 have demonstrated oxalate secretion, while endogenous renal oxalate clearance assessments using direct measurements of serum and urine oxalate have demonstrated net reabsorption. In slc26a6 null mice, the excessive serum oxalate appears to be driven largely by hyperoxalemia rather than by renal leak of oxalate. This disease is extreme and is related to frequent stone recurrence and impaired kidney function. Enteric hyperoxaluria because of inflammatory bowel disease, jejunoileal bypass, and fashionable bariatric surgical procedures for morbid weight problems are the commonest causes of hyperoxaluria in scientific apply. A comparability of Oxalate and calcium are each important in elevating CaOx supersaturation in urine. Normal urine is commonly supersaturated with CaOx as a result of the solubility of CaOx in an aqueous answer is proscribed to approximately 5 mg/L at a pH of 7. Considering that standard urine quantity ranges from 1 to 2 L/day, regular urinary excretion is greater than forty mg. In most instances, one can surmise that ordinary urine is supersaturated with CaOx salt. However, beneath regular circumstances, the blood is undersaturated with respect to CaOx. Over the previous 4 decades, the typical CaP content material of stones has progressively increased. It has been advised that urinary pH elevation plays an important role in the transformation of CaOx to CaP. A retrospective examine of sixty two sufferers discovered that prime urinary pH was the first physiologic abnormality in those in whom CaOx reworked to CaP. This has been supported by experimental proof demonstrating the presence of macromolecules Hyperuricosuria can be because of genetic, metabolic, or dietary factors. The illness manifestations generally current during childhood; nevertheless, they remain silent till puberty. It has been shown that one third of the stones are composed of uric acid, an incidence is greater than the incidence of 8% to 10% reported within the general population. The nature and supply of these putative natural acids is unknown at current but doubtless has an enterohepatic origin. Ectopic fat is termed steatosis, and the sick results of steatosis are termed lipotoxicity,489-494 which is the consequence of the accumulation of toxic metabolites corresponding to acyl coenzyme A (acyl CoA), diacylglycerol, and ceramide. The current belief is that each one cases of traditional and isolated cystinuria are as a end result of mutations in system b0,+. In contrast, clearance of cationic amino acids is only partly affected (40 to 60 mL/min/1. The prevalence is reported to be highest in people of Libyan Jewish descent (1: 2500). A historical past of parental consanguinity might or may not be current because compound heterozygotes can come from apparently unrelated marriage partners. The options that increase suspicion are family historical past of cystinuria, staghorn calculi, positive nonquantitative screening take a look at with sodium nitroprusside (>75 mg/L, zero. Poor cystine solubility and precipitation can typically lead to misleadingly low results, so alkalinization of collected urine is often required. These issues led to the development of a solid-phase assay, which is dependable within the presence of thiol drugs. These stones are quickly rising, department and enlarge, and fill the renal accumulating system to form staghorns. Even with surgical elimination, any remaining fragments containing the infecting bacteria furnish a nidus for further rapid stone development. The nature of those stones to develop rapidly, recur, and trigger morbidity and mortality has led to the time period stone cancer. Chronic urinary stasis or infections predispose to struvite stones so that older age, neurogenic bladder, indwelling urinary catheters, and urinary tract anatomic abnormalities are all predisposing elements. The presence of large stones in contaminated alkaline urine ought to alert the clinician to the potential presence of struvite. Given their potential for fast growth and substantial morbidity, early detection and eradication are essential. With profitable antimicrobial therapy of the underlying an infection, the struvite can really dissolve as a result of the urine is mostly undersaturated with respect to struvite. Whether a stone will dissolve with extended antibiotic is dependent on the amount of carbonate apatite. While many bacteria (gram-negative and gram-positive), Mycoplasma, and yeast species can produce urease, most urease-producing infections are brought on by Proteus mirabilis. Colony counts may be low so the laboratory ought to be instructed to determine any micro organism and decide sensitivities, regardless of how low the variety of colony-forming items. If routine urinary cultures are unfavorable however a urease producer is suspected, the laboratory must be particularly instructed to tradition for Mycobacterium or Ureaplasma urealyticum, which are also urease-positive. Xanthine stones are present in about one third of topics with classic xanthinuria, which is an inborn error in metabolism inherited as an autosomal recessive trait. Patients have very low serum urate ranges but endure from elevated ranges of xanthine in the urine, resulting in xanthine stones, hematuria, and typically occult kidney failure. Xanthine stones occur more typically than hypoxanthine because of the decrease solubility of xanthine in urine. Xanthinuria ought to be suspected if a affected person has important hypouricemia and hypouricosuria in the presence of radiolucent stones. Xanthine stones can also be acquired following allopurinol treatment in patients with vital hyperuricemia similar to Lesch-Nyhan syndrome and in those undergoing chemotherapy for myeloproliferative disorders. Acquired causes may be iatrogenic with using medicines or may be brought on by toxins or other ailments. Melamine is an organic nitrogenous compound used within the industrial productions of plastics, dyes, fertilizers, and materials. The outcomes confirmed that those with high publicity had an increased incidence of urolithiasis. The group of youngsters with kidney stones was reported to be significantly youthful than these without. The challenges include phenocopy, multiple loci, locus heterogeneity, and lack of an intermediate phenotype in scientific databases. In a cross-sectional, population-based research, immigrants of varied ethnic backgrounds maintained their this approach relies on educated guesses of suspected loci.
Order abana 60pills with visaThe scarring is usually separated by regular regions of the kidney and normalappearing calyces does cholesterol medication help weight loss order cheapest abana and abana. The regions of scarring could also be echogenic in comparison with the adjoining regular kidney improve cholesterol levels quickly cheap abana on line. Excretory phase photographs best delineate the extent of involvement cholesterol definition wikipedia best abana 60 pills, especially within the coronal format cholesterol stones order abana 60 pills without prescription. The infections may also be seen in different belly organs- liver, spleen, and adrenals. Typically, renal cysts are asymptomatic and cortical in location; they may be single or multiple. Their cause is unknown, although tubular obstruction has been postulated to be a essential factor. Renal masses produce variable findings on imaging studies, relying on their location. D, T2-weighted picture after remedy exhibits distorted, dilated calyces containing particles. Complex cysts contain proteinaceous or hemorrhagic fluid and should have septations and calcification. The T1 signal intensity of the fluid is higher than anticipated for simple fluid, ranging from isointense to hyperintense. T2 signal depth is decrease than anticipated for simple fluid and may be black, depending on the blood content material. The corticomedullary distinction is misplaced with diffuse elevated cortical echogenicity. A fluid degree may be visible as a outcome of the presence of debris or hemorrhage inside some of the cysts. Thekidneysare equally enlarged, and the a quantity of various-sized cysts contain bothkidneys. Solid lesions smaller than 3 cm in diameter might represent both adenomas or renal cell carcinomas, whereas most lesions bigger than three cm are renal cell carcinomas. The cystic spaces predispose to stasis, which finally ends up in stone formation and potential infection. Involvement is usually bilateral, although not always symmetric, with as few as one calyx involved. The kidneys are sometimes normal sized with an look of medullary nephrocalcinosis when small stones are present. With extra extreme involvement, the cystic dilations may seem grapelike or beadlike. T2-weighted coronal picture shows diffuse atrophy and multiple cysts in a patient on chronicdialysis. Multicystic dysplastic kidney is an uncommon, congenital, nonhereditary condition. It may be difficult to differentiate this condition from extreme hydronephrosis if no cyst partitions or septa are seen. On contrast material�enhanced research a calyceal diverticulum appears as a small round or oval assortment of distinction materials linked to the fornix of the calyx. Although a few of these lesions are benign, surgical procedure may be essential for prognosis and therapy. D, Maximum-intensity projection depicts the multiple renal massesinangiographicformat. Acysticmass is visible within the left kidney with an inside stable element in the lowerpole. The left lower pole cystic lesion proved to be a renal cell carcinoma, papillarytype. Renal neoplasms may come up from either the renal parenchyma or the urothelium of the pelvicalyceal system. With the elevated use of cross-sectional imaging strategies, extra small neoplasms are discovered incidentally. In uncommon circumstances, only a minimal amount of fat is current, and it must be looked for diligently. Opposed-phase chemical shift sequences cause an "India ink" define of the tumor at its interface with regular renal parenchyma. Oncocytoma is an uncommon benign tumor originating within the epithelium of the proximal accumulating tubule. A, Gray-scale ultrasonogram reveals a posh cyst withasolidnodularcomponent(arrow). The nodule (arrow) reveals dense arterial phase enhancement with heterogeneous washout. The lesion was subsequently resected and was discovered to be a transparent cell carcinoma, Fuhrmangrade2. Renal cell carcinoma is the third commonest tumor of the genitourinary tract after carcinoma of the prostate and bladder. After the injection of intravenous contrast materials, most renal cell carcinomas present enhancement. The heterogeneity will increase with increasing measurement because of variable quantities of necrosis and intraluminal lipid. The intraluminal lipid could make areas of the mass drop in signal intensity on opposed-phase T1-weighted sequences. The staging of renal cell carcinoma is essential in predicting survival rates and planning the proper surgical method to the mass. Both the World Health Organization and the Robson classifications are used within the staging of renal cell carcinoma. A, T2-weighted picture reveals a heterogeneous, brilliant mass on the left with a well-defined pseudocapsule. B, T1-weighted picture confirms a well-defined darkish mass involvingtheleftrenalcortex. Transitional cell carcinoma of the bladder is far more common than that of the kidney or ureter. The imaging findings are much like those of renal cell carcinoma, except the lesions tend to not enhance as much on postcontrast imaging. Evaluation of the entire amassing system is required as a outcome of synchronous lesions could also be current. Coronal(A)andaxial(B)T2-weightedimagesshowa heterogeneous mass within the lower pole of the left kidney with infiltration of the perinephric fat and extensive retroperitoneal lymphadenopathy. Lymphoma might contain the kidney as a half of multiorgan involvement or, in rare instances, as a major neoplasm. An infiltrative picture with lymphomatous substitute of the kidney can also be noticed. Lymphoma usually seems hypointense on T1-weighted sequences and heterogeneous to slightly hypointense on T2-weighted sequences. Treated lymphoma might differ in sign intensity, as a outcome of the effects of therapy. Intravenous administration of furosemide has been proposed to enhance urine clearance from the renal collecting system, although the exact benefit of such intervention in enhancing lesion detection stays undefined. Coronal (C) and axial (D) gadolinium-enhanced T1-weighted pictures show enhancing material within dilated calyces and pelvis of the decrease pole moiety (arrow). In fact this study instructed that 11C-acetate may be useful in differentiating "fat-poor angiomyolipoma" from renal cell cancer with a sensitivity of 93. A, Coronal T2-weighted picture reveals a large, infiltrating left renal mass extending into the perirenal fats. Thepositronemission tomographic scan (C) exhibits hypermetabolism at the periphery of the large renal mass and inside the pulmonary nodules. Variant anatomy may be a problem; accent renal arteries, which happen in 15% to 20% of affected sufferers, is most likely not imaged. Sensitivity and specificity for the methods have generally been in the vary of 50% to 70%. The main renal artery, as well as its segmental branches, could be viewed and evaluated. Axial (A) and coronal (B) slab maximum-intensity projection pictures show the atherosclerotic stenosis of the proximal renal artery.
Cheap 60 pills abana overnight deliveryThe detection of IgAfibronectin complexes was initially thought to be a marker in patients with IgA nephropathy cholesterol lowering diet heart foundation discount abana 60pills overnight delivery, however it has not confirmed to be a useful medical check cholesterol units order abana 60pills online. This phenomenon occurred in 10% to 15% of sufferers and possibly suggests sensitivity to bovine serum albumin usda cholesterol in eggs generic abana 60pills overnight delivery. Levels of complements cholesterol levels post mi purchase abana 60pills online, such as C3 and C4, are usually regular and, in some patients, even elevated,949 as are complement components C1q, C2-C9. In this regard, C3 fragments are increased in 50% to 75% of sufferers,951,952 and C4-binding protein concentrations are also increased. Mesangial and endocapillary hypercellularity, segmental glomerulosclerosis, and extracapillary proliferation are strongly associated with proteinuria. The latter is often reserved for these sufferers with documented progressive disease. Although prednisone was initially thought of to be with out effect,870 some cohort studies have instructed that corticosteroids might afford some profit. These sufferers have nephrotic-range proteinuria and diffuse foot course of effacement. More aggressive treatment may be applicable in sufferers with severe crescentic or progressive IgA nephropathy. Of concern, nevertheless, was the discovering in 12 sufferers of the persistence of crescents on repeat biopsy, regardless of the early and aggressive remedy with pulse methylprednisolone and oral prednisone, and a short-term reversal of the acute crescentic glomerulonephritis. Other Modalities Aliskiren, a direct inhibitor of renin, has received attention of late as an antiproteinuric agent in IgA nephropathy. An open-label pilot study in 25 consecutive patients with IgA nephropathy in Hong Kong handled for 12 months with aliskiren resulted in a 26. Of observe, it has since been proposed that the obvious lack of good thing about cyclophosphamide remedy could have been clouded by the potential danger of a just lately recognized mechanism of acute kidney injury in study subjects, termed warfarin-related nephropathy. With regard to azathioprine use, a randomized controlled trial in Italy of 207 patients with biopsy-proven IgA nephropathy compared steroids alone or together with azathioprine for six months and found no difference in renal survival, defined as time to 50% improve in plasma creatinine from baseline over a median follow-up of four. Similarly, in a multivariate analysis1017 specializing in the subgroup of 70 patients from the identical cohort with a baseline serum creatinine concentration of more than 1. Another retrospective evaluation,1013 nonetheless, showed no good thing about tonsillectomy on the clinical course of IgA nephropathy. Although urinary protein excretion was considerably larger within the tonsillectomy group on the 12-month mark (P < zero. In those sufferers with progressive renal insufficiency, the utilization of prednisone and cyclophosphamide adopted by azathioprine must be considered. Although graft loss because of recurrent IgA nephropathy is type of unusual (<5%),1033 a recurrence of IgA nephropathy worsens the overall prognosis for long-term survival of an allograft,1034,1035 particularly if crescentic illness is current. In a research by the Mayo Clinic1021 106 patients had been randomly assigned to either 12 g of -3 fatty acids or olive oil for two years. Only 6% of patients handled with fish oil experienced a doubling of their plasma creatinine concentration, in contrast with 33% of those handled with olive oil. The enthusiasm for this strategy, however, was tempered by subsequent studies that confirmed no advantage of fish oil therapy. A minority of pathologists, nonetheless, advocate grouping glomerular diseases with both fibrillary deposits or microtubular deposits beneath the time period immunotactoid glomerulopathy. In capillary partitions, the fibrillary deposits could be subepithelial, subendothelial, or intramembranous. Note the random orientation of the former and the microtubular look and greater organization of the latter. By the method illustrated, fibrillary glomerulonephritis is distinguished from immunotactoid glomerulopathy based on the ultrastructural characteristics of the deposits. The fibrils are distinctly larger than the actin filaments in adjoining cells, which is a helpful remark that helps distinguish the fibrils of fibrillary glomerulonephritis from these of amyloidosis, which are only slightly larger than actin. Most patients with fibrillary glomerulonephritis have substantial proteinuria, and therefore there normally is in depth effacement of visceral epithelial foot processes. Light Microscopy In fibrillary glomerulonephritis, extensive localization of fibrils in capillary partitions causes capillary wall thickening. Mesangial localization causes elevated mesangial matrix and usually stimulates mesangial hypercellularity. Varying distributions of the fibrillary deposits trigger the sunshine microscopic appearance of fibrillary glomerulonephritis to be extremely variable. Of seventy four sequential fibrillary glomerulonephritis specimens evaluated at University of North Carolina, 28% had crescents with a mean involvement of 29% of glomeruli (range, 5% to 80%). Combined capillary wall thickening and mesangial growth is commonest, which often offers a membranoproliferative appearance. Immunotactoid deposits could additionally be large, leading to nodular mesangial enlargement in some specimens. Immunofluorescence Microscopy the deposits of fibrillary glomerulonephritis almost all the time stain extra intensely for IgG than for IgM or IgA, and lots of specimens have little or no staining for IgM and IgA. It is neither granular nor linear; as an alternative, it has an irregular bandlike appearance in capillary walls and an irregular shaggy appearance in the mesangium. Fibrillary glomerulonephritis and immunotactoid glomerulonephritis have been associated with lymphoproliferative illness. Rarely, fibrillary glomerulonephritis could additionally be related to concomitant hepatitis C virus infection1051 or an unusual IgM glomerular deposit disease. The microtubules of immunotactoid glomerulopathy even have a larger tendency to align in parallel arrays, whereas the fibrils of fibrillary glomerulonephritis all the time are randomly distributed. However, cryoglobulinemic microtubules sometimes are shorter and fewer properly designed than immunotactoid microtubules. Patients with fibrillary glomerulonephritis current with a mixture of nephrotic and nephritic syndrome features. In a collection of 28 patients with fibrillary glomerulonephritis seen on the University of North Carolina, the mean age was forty nine years (range, 21 to 75 years), the ratio of males to females was 1: 1. At presentation, 100% of patients had proteinuria, 52% had hematuria, 71% have been hypertensive, and 66% had renal insufficiency. Underlying malignancy (23%), dysproteinemia (17%), and autoimmune disease (15%) were frequent. Such patients have progressive renal failure in lower than 5 years, though long-term affected person survival is greater than 80% at 5 years. In the most important series to date, sixteen patients with immunotactoid glomerulopathy have been recognized from the pathology archives at Mayo Clinic in Rochester, Minnesota. Proteinuria was current in one hundred pc of sufferers; 80% had microhematuria, 69% had nephrotic syndrome, and 50% had renal insufficiency. There have been no statistically significant differences in medical presentation between patients with fibrillary glomerulonephritis and people with immunotactoid glomerulonephritis. Etiologically, sufferers with immunotactoid glomerulonephritis have been statistically extra more doubtless to have an underlying lymphoproliferative illness, a monoclonal spike on serum protein electrophoresis, and hypocomplementemia. One small case collection (three patients) reported significant enchancment in proteinuria in response to rituximab (either alone or together with corticosteroids) or tacrolimus. One report describes recurrent disease in three of four patients who had acquired 5 transplants. This pathologic function could be seen on mild, immunofluorescence, and electron microscopy. Two examples are acute thrombotic microangiopathy and atheroembolic kidney illness. The incidence of quickly progressive glomerulonephritis has been estimated to be as low as seven circumstances per million population per 12 months. Immune complex crescentic glomerulonephritis is caused by immune complicated localization inside glomeruli. The presence of microangiopathic hemolytic anemia and thrombocytopenia are indicators that the rapid loss of kidney operate is more likely brought on by hemolytic uremic syndrome than crescentic glomerulonephritis. Frequency is set with respect to age in sufferers whose kidney biopsy specimens have been evaluated at the University of North Carolina Nephropathology Laboratory. The pattern and composition of immunoglobulin and complement staining depend upon the underlying category of immune advanced glomerulonephritis or C3 glomerulopathy that has induced crescent formation.
Order discount abana on-lineThe combination of M cholesterol ratio risk generic abana 60 pills mastercard, S cholesterol levels in chronic kidney disease order 60 pills abana fast delivery, and T lesions with clinical parameters significantly increased the flexibility to predict development within the absence of substantial immunosuppressive therapy cholesterol levels after quitting smoking discount 60 pills abana with visa. Studies to date have been retrospective and thus prospective research using the Oxford classification are warranted cholesterol test ireland discount 60 pills abana fast delivery. Rather, it pertains to an anomaly in the IgA molecule itself, specifically, in its glycosylation, as discussed earlier. O-linked monosaccharides or oligosaccharides consisting of N-acetylgalactosamine could be posttranslationally added to these amino acid residues. Three mechanisms have been postulated: extreme exercise of 2,6-sialyltransferase, decreased exercise of 1,3-galactosyltransferase, and decreased stability of 1,3galactosyltransferase due to decreased exercise of its chaperone (Cosmc). This neoepitope is the goal of IgG autoantibodies as demonstrated in studies of immortalized B cells from sufferers with IgA nephropathy,824,828 and IgG autoantibodies particular for Gd-IgA1 are discovered in the circulation of such patients. A latest study demonstrated that serum levels of IgG- and IgA-based antiglycan autoantibodies from ninety seven sufferers with IgA nephropathy, compared to 30 patients with non-IgA nephropathy disease and 30 healthy controls, correlate with illness development and poor prognosis. Formation of circulating immune complexes with abnormally glycosylated IgA and circulating IgA receptor molecules may be concerned. A number of autoantibodies to varied putative autoantigens have been described in IgA nephropathy. The episodes are inclined to occur in shut temporal relationship to upper respiratory an infection, together with tonsillitis or pharyngitis. This synchronous association of pharyngitis and macroscopic hematuria has been given the name synpharyngitic nephritis. Much much less generally, episodes of macroscopic hematuria observe infections that contain the urinary tract or gastroenteritis. Macroscopic hematuria could also be totally asymptomatic however more typically is associated with dysuria that may prompt the treating physician to contemplate bacterial cystitis. Systemic symptoms are frequently discovered, together with nonspecific symptoms similar to malaise, fatigue, myalgia, and fever. When it happens in older people, it ought to increase the potential for the extra widespread causes of urinary tract bleeding, such as stones or malignancy. A presentation with asymptomatic microscopic hematuria, with or without proteinuria, happens in 30% to 40% of sufferers. Patients with IgA nephropathy come for analysis of asymptomatic hematuria with or without the presence of proteinuria. In addition to having glomerulonephritis, these sufferers might generally have hypertension. In fact, in white sufferers with hypertension and hematuria, IgA nephropathy is the commonest form of hematuria. Microscopic hematuria and proteinuria persist between episodes of macroscopic hematuria. Patients with nephrotic syndrome at presentation may have widespread proliferative glomerulonephritis or coexisting IgA nephropathy and minimal change glomerulopathies. These people sometimes have had asymptomatic microscopic hematuria and proteinuria that has remained undetected. In a review encompassing 1900 patients derived from eleven separate series, long-term renal survival was estimated to be 78% to 87% at a decade after presentation. A poor end result was associated with persistent hematuria, microalbuminuria, and tubulointerstitial modifications on the kidney biopsy specimen. This study clearly demonstrates that careful follow-up is required for all patients given the prognosis of IgA nephropathy. Patients with episodes of gross (macroscopic) hematuria generally have a extra favorable prognosis than those with persisting microhematuria; however, after an episode of microhematuria associated with acute renal failure a portion of sufferers (about 25%) could not get well normal kidney operate. Sustained hypertension, persistent proteinuria (especially proteinuria of >1 g protein per 24 hours), impaired kidney perform, and nephrotic syndrome are markers of poor prognosis. Alternatively, macroscopic hematuria may represent an episodic process that leads to self-limited irritation, in contrast to persistent hematuria that represents ongoing, low-grade inflammation. The fact that acute renal failure does occur throughout gross episodes of hematuria has been confirmed. After the episodes of gross hematuria, kidney function usually returns to baseline and the long-term prognosis is good. The degree of proteinuria is greater than likely a further marker of glomerular illness. In a research by Chen and colleagues,884 mice that had been made proteinuric by numerous methods had enhanced deposition of administered IgA immune complexes. This suggests that these complexes could be more easily deposited in proteinuric states. The Toronto formulation primarily based on common imply arterial strain and proteinuria in the course of the first 2 years of remark is one of the best validated in white American and European subjects,886 however a large fraction of the variation in progression stays unexplained by these two factors. In addition to these variables, weight problems,908 elevated nocturnal blood pressure,909 increased uric acid ranges,909 and elevated ranges of C4-binding protein910 have been related to a poorer prognosis. Moderate alcohol consumption is associated with an improved prognosis in IgA nephropathy. Prolonged, high-level exposure to natural solvents may also confer a worse prognosis to sufferers with IgA nephropathy. The infant survival rate was 93% on this examine; preterm delivery occurred in nearly two thirds and progress retardation in a single third of infants. The identification of abnormally galactosylated IgA1 has led to the development of a possible diagnostic take a look at based mostly on the detection of elevated lectin binding in sufferers with IgA nephropathy. Immune complex�mediated glomerulonephritis and C3 glomerulopathy normally have various combinations of capillary wall thickening and endocapillary hypercellularity in the intact glomeruli. The hallmark ultrastructural finding is immune complex�type electron-dense deposits. These deposits can be mesangial, subendothelial, intramembranous, subepithelial, or any combination of these. The pattern and distribution of deposits could point out a selected phenotype of main crescentic immune complex glomerulonephritis, similar to postinfectious, membranous, membranoproliferative, or dense deposit illness. For example, endothelial tubuloreticular inclusions recommend lupus nephritis, and microtubular configurations in immune deposits suggest cryoglobulinemia. Dense fibrin tactoids happen in thrombosed capillaries, in sites of fibrinoid necrosis, and within the interstices between the cells in crescents. Multiple causes and pathogenic mechanisms can result in the ultimate common pathway, together with many kinds of immune complicated illness. The general dogma is that immune advanced localization in glomerular capillary partitions and mesangium, by either deposition or in situ formation or both, activates a quantity of inflammatory mediator techniques. The activated cells also release soluble mediators, similar to cytokines and chemokines. Complement activation has typically been thought of a serious mediator of injury in immune advanced glomerulonephritis; however, experimental data additionally point out the significance of Fc receptors in immune complex�mediated injury. The second peak is in the sixth and seventh many years, and this later-onset disease is extra widespread in girls, who more often have renallimited disease. Nephritis-sensitive mouse strains had kallikrein haplotypes that were distinct from those of management strains, together with several regulatory polymorphisms. The scientific knowledge and lightweight microscopic findings ought to assist make this distinction. Glomeruli with crescents sometimes have fibrinoid necrosis in adjoining glomerular segments. Nonnecrotic segments may look totally normal by gentle microscopy or might have slight infiltration by neutrophils or mononuclear leukocytes. This differs from crescentic immune advanced glomerulonephritis and C3 glomerulopathy, which usually have capillary wall thickening and endocapillary hypercellularity within the intact glomeruli. Because extra severe instances of immunoglobulin A nephropathy and postinfectious glomerulonephritis are extra typically evaluated by kidney biopsy, the extent of crescent involvement is greater within the sufferers included on this desk than in the basic group of sufferers with these diseases. The acute necrotizing glomerular lesions and the mobile crescents evolve into glomerular sclerosis and fibrotic crescents, respectively. There also is focal tubular epithelial acute simplification or atrophy, focal interstitial edema and fibrosis, and focal interstitial infiltration of predominantly mononuclear leukocytes. Electron Microscopy the findings by electron microscopy mirror these seen by gentle microscopy.
Buy abana with mastercardOn the other hand cholesterol good for you purchase abana 60 pills free shipping, perioperative eculizumab remedy would possibly defend the liver from thrombotic microangiopathy and shield towards early failure by preventing uncontrolled complement activation precipitated by surgical stress and revascularization damage exogenous cholesterol definition order genuine abana. Thus cholesterol hdl buy generic abana, liver transplantation cholesterol medication pravastatin purchase 60 pills abana, underneath the umbrella of perioperative eculizumab remedy, may be a valuable choice when chronic eculizumab therapy is unfeasible because of safety issues or useful resource restriction. Patients with cobalamin C deficiency often present within the early days and months of life with failure to thrive, poor feeding, and vomiting. Children might present neurologic symptoms of fatigue, delirium, psychosis, and seizures. In circumstances with early onset, the illness has a fulminant evolution and occasionally includes the pulmonary vasculature, but when it ensues later in childhood it could comply with a more persistent course. The hallmarks of defective cobalamin C metabolism are hyperhomocysteinemia and methylmalonic aciduria, and the extremely high homocysteine ranges (up to tenfold higher than normal) have been suggested to have a task within the pathogenesis of the vascular lesions. Without therapy, the disease is deadly, and some children probably die undiagnosed. Daily intramuscular administrations of hydroxycobalamin may reduce homocysteine levels and methylmalonic aciduria, whereas oral hydroxycobalamin and cyanocobalamin are ineffective. Oral betaine helps cut back serum homocysteine levels further by activating betaine homocysteine methyltransferase. Folic acid supplementation to avoid folate deficiency induced by methyltetrahydrofolate trapping and L-carnitine to enhance propionyl carnitine excretion have been suggested, however their role in improving disease outcome is unclear. Intensified therapy in older youngsters with less acute disease could achieve remission of the microangiopathic course of and amelioration of the other medical manifestations of the metabolic dysfunction. This protein performs a serious position in main hemostasis by forming platelet plugs at the sites of vascular injury under high shear stress. Eleven cases have been reported during treatment with clopidogrel, a new antiaggregating agent that has achieved widespread medical use for its safety profile. The total survival fee is 67% and is improved by early therapy withdrawal and plasma therapy. Plasma manipulation is a cornerstone within the therapy of the acute episode (see Table 35. Plasma may serve to induce remission of the disease by replacing faulty protease exercise. Rituximab has been additionally used electively to stop relapses in patients with autoantibodies and recurrent disease. Three sufferers maintained a disease-free status after 29, 24, and 6 months, respectively. Studies on secretion and activity of the mutated types of the protease have shown that the majority of those mutations lead to an impaired secretion from cells and, when the mutated protein is secreted, the proteolytic activity is greatly decreased. In most cases, eculizumab will obtain prompt remission of signs and signs of the microangiopathic process, and plasma trade will now not be required. However, should extra change classes be indicated, further eculizumab doses ought to be administered shortly after each process because the drug is totally cleared from the circulation in the course of the trade. Fresh-frozen plasma, 1 or 2 L, must be exchanged day by day till full and sustained remission of the microangiopathic course of has been obtained (see Table 35. The length of remission has ranged from 9 months to four years, with relapses reported in roughly 10%. Dialysis is required in 28% to 61% of patients with acute or subacute illness, with 20% to 30% recovering some kidney perform after a variable interval of dialytic support. The differential analysis includes systemic vasculitis, subacute bacterial endocarditis, polymyositis, myoglobinuric renal failure, drug-induced interstitial nephritis, and renal artery thrombosis or thromboembolism. Atheroembolic renal disease can also occur in renal allografts, with a frequency starting from zero. The early form is often related to primary nonfunction, and the embolic illness is confined to the allograft. The second type is a late medical presentation, which may come up years after transplantation in steady grafts. The disease is often associated with precipitating elements, and in some instances shows options of a systemic disorder. Early presentation is incessantly associated with poor prognosis, whereas late manifestations typically have a extra benign course. The elongated clefts are actually voids where ldl cholesterol crystals were positioned before fixation and staining. Note the exuberant intimal thickening and the cellular proliferation, which fully occlude the lumen. B, Electron micrograph exhibiting needle-like clefts from atheroemboli to afferent arterioles. To scale back the danger of atheroemboli, an accurate assessment of organ donors must be accomplished. At the time of organ procurement, manipulation of the aorta should be stored to a minimal, mobilizing the kidneys without cross-clamping the aorta, as carried out for residing related donors. Proteinuria is current in more than 50% of sufferers and will sometimes be in the nephrotic range. The subsequent intravascular inflammatory reaction has been studied in experimental models of atheroembolism and in human biopsy and autopsy samples. In the chronic part, tissue ischemia is perpetuated by marked endothelial proliferation, intimal thickening, concentric fibrosis of the vessel wall, and persistence of cholesterol crystals and big cells in the lumens of affected arteries. Hyalinization of glomeruli, atrophy of renal tubules, and multiple wedge-shaped infarcts within the kidney result in reduced kidney size. These events induce a general inflammatory response, including the recruitment of neutrophils and macrophages to the location of crystal formation. Although these enhance local irritation, macrophages may contribute to crystal clearance or progressive scarring, respectively. Also, the brachial strategy for aortography or coronary angiography seems to be burdened by less morbidity than the femoral approach. Because kidney irritation is minimal or absent on radiation publicity, the time period radiation nephritis initially introduced to describe this clinical entity has been progressively replaced with the extra appropriate term, radiation nephropathy. Modern radiation remedy is sharply targeted on the realm to be treated; due to this fact, it is extremely unlikely that the kidneys would be irradiated in a case of irradiation for uterine cervical most cancers or prostate cancer. Patients manifest arteriovenous nicking on funduscopic examination, normochromic normocytic anemia, microscopic hematuria, proteinuria, and urinary casts. Renal perform decreases progressively, with significant proteinuria and microscopic hematuria, with or without casts. Kidney perform decreases slowly, with a biphasic pattern in most sufferers, with persistent decline in the first 12 to 24 months, followed by a interval of stabilization. Late Malignant Hypertension this condition arises 18 months to eleven years after irradiation in sufferers with continual radiation nephropathy or benign hypertension. Glomerular capillary endothelial cell loss and mesangiolysis are noticed inside weeks after irradiation. Late changes include discount in whole renal mass, with prominent and sclerosed interlobar and arcuate arteries, glomerular capillary loop occlusion and hyalinization, with progressive tubular atrophy, elevated mesangial matrix, mesangial sclerosis and, finally, glomerulosclerosis. Irradiation for neoplastic illnesses of the pelvis, in particular for the treatment of malignant seminomas, has traditionally been the main reason for radiation nephropathy. This explains why, in parallel with the progressive substitute of irradiation with pharmacologic remedy for this illness, the incidence of radiation nephropathy has been progressively declining over time. In newer years, nevertheless, the incidence of the disease again began to improve, together with the rapidly growing use of total physique irradiation of candidates for bone marrow transplantation. It has been advised that chemotherapy administered as part of the preparative regimen may potentiate the consequences of irradiation on the kidneys. Most of the theories proposed to clarify the pathogenesis of radiation nephropathy are based on murine research. Diffuse apoptosis and lysis of tubular cells, with totally different degrees of proliferation of the residual cells, is one other attribute pattern of radiation nephropathy. Apoptosis early after 5-Gy, single-dose, total body irradiation has been demonstrated in rats, adopted by a late proliferative response. Thus, preventive measures to be noticed in the course of the administration of radiation therapy are of paramount significance to restrict or forestall opposed effects on the kidney. These embrace selective shielding of the kidneys and using minimal effective doses of fractionated radiation, when potential. Clinical Features the pattern of presentation could vary from restricted to diffuse cutaneous involvement. |